
The right sports therapy exercises are not the hardest ones. They are the ones that match your injury, your current capacity, and the job you need your body to do next.
Sports rehabilitation exercises can reduce pain, restore motion, rebuild strength, and prepare you for return to training. They can also flare symptoms if the exercise is wrong for the tissue, the phase of healing, or the way you move. This guide explains the common categories, how physiotherapy exercises are progressed, what you may be able to do at home, and when an in-person assessment makes more sense. This is general education, not a diagnosis or a personalized rehab plan.
What sports therapy exercises are and who they help
Sports therapy exercises are movement-based rehab tools used to restore mobility, strength, balance, control, and confidence after injury, surgery, or persistent pain. They are used across early recovery, later strengthening, and return-to-sport planning, but the best choice depends on the tissue involved, symptom irritability, healing stage, sport demands, and your biomechanics.
Physiotherapy exercises help more than competitive athletes. They also help runners, lifters, court-sport players, active office workers, and post-surgical patients who want to move normally again. A generic physical therapy exercises list can be useful for ideas, but it cannot tell you whether your issue is load intolerance, stiffness, weakness, poor control, or the wrong movement pattern.
How to choose the right rehab exercise for your stage of recovery
The safest framework is phase-based, not exercise-by-exercise copying from social media. Early rehab usually focuses on settling pain and swelling, restoring basic range of motion, and building tolerance with low-load isometrics or simple patterning. Mid-stage rehab usually shifts toward strength, control, and tissue capacity with bodyweight or external load. Later rehab adds impact tolerance, faster force production, deceleration, cutting, and return to sport exercises when the basics are solid.
Progression works best when symptoms stay tolerable during the session and do not spike later the same day or the next day. That is why one athlete may start split squats early while another needs bridge work, assisted sit-to-stands, or pool exercise first. Post-surgical plans and tendon injuries often need stricter sequencing, so online rehab exercises for athletes should never override a surgeon’s protocol or clinician guidance.
Red flags: when not to exercise and when to get medical advice
Stop and get medical review if an injury leaves you unable to bear weight, if a joint locks, if major swelling appears quickly, or if the limb repeatedly gives way. Urgent assessment is also appropriate for sudden severe weakness, unexplained numbness, bowel or bladder changes, fever with pain, chest pain, or shortness of breath.
Normal rehab discomfort is usually mild and settles. Sharp pain, repeated instability, rapidly increasing swelling, or a clear loss of function after exercise is different. If symptoms persist, or if you are trying to return to running, lifting, or sport and are not sure what is safe, an in-person assessment can narrow down the right loading strategy. In downtown Toronto, that usually means a sports physio or sports medicine assessment rather than guessing from a PDF.
Core exercise categories used in sports rehab

Most sports therapy exercises fall into five groups: mobility, strength, balance and proprioception, trunk control, and conditioning. A simple starting dosage for educational examples is often 1 to 3 sets of 6 to 15 reps or 10 to 30 second holds, adjusted to symptom response and movement quality.
Mobility work targets stiffness, guarded movement, and joint range. Strength work can start with isometrics, then progress to slow controlled isotonic loading, then heavier or faster loading. Balance and proprioception exercises train position sense and control, especially after ankle, knee, and hip injuries. Core work improves force transfer and trunk control. Low-impact cardio during recovery helps maintain conditioning when running or jumping is not yet tolerated.
Full body physical therapy exercises can be useful when deconditioning, surgery, or time away from sport affects more than one area. But body-part specific rehab still matters when the issue is localized, such as an ankle sprain, rotator cuff weakness, or tennis elbow.
Sports therapy exercises by body area

Shoulder rehab exercises
Shoulder rehab often starts with scapular control, rotator cuff isometrics, supported rows, and wall slides. A common educational dosage is 2 to 3 sets of 6 to 12 reps or 20 to 30 second holds. These drills target cuff loading, shoulder blade control, and tolerance for reaching.
A regression is a lower arm angle, lighter band, or supported position against the wall or table. A progression is heavier rowing, controlled carries, incline pressing, or overhead work if range and control allow. Common mistakes are shrugging, arching the low back, and pushing into a painful overhead range too soon.
Neck rehab exercises
Neck pain often responds better to low-load control than aggressive stretching. Deep neck flexor drills, gentle mobility, postural endurance, and scapular support work are common physiotherapy exercises for neck pain. A broad starting point is 2 to 3 sets of short holds or 6 to 10 slow reps.
A regression is unloading the position or reducing range. A progression is longer holds, resisted work, or adding arm movement while keeping the neck relaxed. Common mistakes are clenching, jutting the chin, and moving too far into symptom-provoking positions.
Back rehab exercises
Back pain rehab usually works best when the exercise matches the movement pattern you tolerate. Breathing and bracing drills, hip hinge patterning, bird dog variations, side bridge variations, and graded mobility are common options. A broad educational range is 2 to 3 sets of 6 to 10 reps or 10 to 30 second holds.
A regression is a shorter lever, smaller range, or supported setup. A progression is adding load, tempo, carries, or more complex hinge and squat patterns. Common mistakes are rushing reps, holding the breath too hard, and forcing a range that the back does not currently tolerate.
Hip and knee rehab exercises
Hip and knee rehab often uses glute bridges, sit-to-stands, split squat patterns, step-ups, hamstring loading, terminal knee extension, and squat progressions. A common educational dosage is 2 to 3 sets of 6 to 12 reps. These drills build quad, glute, and hamstring capacity while improving alignment and control.
A regression is reducing depth, using support, or shifting to bilateral work. A progression is adding load, increasing step height, moving to single-leg patterns, or slowing the eccentric phase. Common mistakes are knee collapse inward, weight shift away from the involved side, and adding depth before control is ready.
Ankle and foot rehab exercises
Physical therapy exercises for legs and feet often include calf raises, ankle mobility, foot intrinsic drills, single-leg balance, and later hopping or landing progressions. A broad starting point is 2 to 3 sets of 8 to 15 reps or 20 to 30 second balance holds. These are central in sprain recovery, Achilles loading, plantar fascia rehab, and return to running.
A regression is double-leg calf raises, fingertip support, or seated loading. A progression is single-leg work, tempo loading, uneven surfaces, eyes-closed balance, or controlled hopping if symptoms allow. Common mistakes are rolling the foot out, rushing balance work, and skipping calf strength because pain has settled.
Elbow and wrist rehab exercises
Wrist extensor loading, grip modifications, forearm control, and shoulder-supported drills are common for elbow and wrist symptoms. A broad educational dosage is 2 to 3 sets of 8 to 12 reps with slow control. That matters in tennis elbow, gym-based overuse, and keyboard-related forearm pain.
A regression is reducing wrist range or using isometrics. A progression is heavier eccentric or isotonic loading, carries, or return to sport drills that reintroduce grip and impact gradually. Common mistakes are gripping too hard, moving too fast, and ignoring the role of shoulder or scapular weakness.
Core-focused rehab exercises
Core rehab is less about endless crunches and more about anti-rotation, anti-extension, breathing, and load transfer. Dead bug patterns, side bridge progressions, carries, and controlled trunk rotation drills are common. A broad dosage is 2 to 3 sets of 6 to 10 reps or 10 to 30 second holds.
A regression is shorter lever length or more support. A progression is band resistance, offset loading, single-leg stance, or sport-specific rotation. Common mistakes are losing rib and pelvis control, over-bracing, and choosing fatigue over quality.
Diagnosis-specific examples athletes actually search for

ACL rehab usually prioritizes knee extension, quad activation, gait mechanics, swelling control, and progressive single-leg strength before later landing and deceleration work. Common examples include quad sets, straight-leg raises if tolerated, sit-to-stands, step-ups, split squats, and later hopping or change-of-direction drills under supervision. Exact timelines vary by surgery, graft, swelling, strength, and surgeon protocol, so generic return-to-sport calendars are not reliable for your case.
Meniscus-related rehab often focuses on extension, swelling control, quad and hip strength, and graded tolerance to loaded knee flexion as appropriate. Common examples include terminal knee extension, controlled squat variations, bridge work, bike intervals, and step-based progressions within tolerated range.
Rotator cuff pain or weakness usually responds to cuff loading, scapular mechanics, and a gradual rebuild of overhead tolerance. Common examples include external rotation isometrics, supported rows, wall slides, carries, and pressing or overhead progressions once control improves.
A sprained ankle usually needs swelling management, range restoration, calf strength, and balance retraining before hopping, cutting, and reactive drills. Common choices are ankle alphabet work, calf raises, dorsiflexion mobility, single-leg stance, step-down control, and later pogo or hop progressions.
Achilles tendinopathy and plantar fasciitis usually respond better to graded loading than full rest. Common examples include calf raises, bent-knee and straight-knee heel raise variations, foot intrinsic work, walking or running load modification, and mobility only where it helps function. Tendon pain and fascia pain can both flare if volume rises too fast, even when one session feels fine.
Tennis elbow rehab usually centres on progressive tendon loading and grip modification, not only forearm stretching. Wrist extensor isometrics, slow eccentrics, pronation and supination control, and shoulder support work are common.
Low back pain that may be disc-related still benefits from movement in many cases, but the tolerated direction and load vary. The useful rehab path is usually graded loading, trunk control, and reducing fear-driven avoidance rather than trying random stretches from a physical therapy exercises PDF.
Home vs clinic vs gym-based rehab

The best setting depends on the stage and the skill required. Home-based physical therapy exercises at home are best for consistency, symptom-management, range-of-motion work, and basic strength. Clinic rehab is best for assessment, movement correction, diagnosis-informed exercise selection, and progressing complex or persistent cases. Gym-based rehab becomes more useful when higher loads, power, and return-to-sport conditioning matter.
| Setting | Best for | Limits | Good examples |
|---|---|---|---|
| Home | Daily consistency, mobility, activation, early strength | Harder to self-correct form | breathing drills, bridges, wall slides, calf raises |
| Clinic | Assessment, supervision, symptom monitoring, technique changes | Less frequent than home work | coached squats, balance retraining, return-to-run progressions |
| Gym | Higher load, power, confidence, athletic capacity | Easy to progress too fast | split squats, loaded carries, sleds, controlled plyometrics |
A blended model works well for many active adults: get assessed once symptoms are not clear, then use a structured home or gym plan between visits. Generic online lists, physical therapy exercises with Pictures, or printable sheets can help with recall, but they are only safe when the exercise matches the actual problem and your current stage.
How often to do sports therapy exercises
Frequency depends on the goal of the exercise. Mobility, gentle activation, and some symptom-management drills may be done daily. Heavier strength or impact work is commonly done 2 to 4 times per week to allow recovery. Balance practice often sits in the middle, with short exposures several times per week.
Quality beats quantity. Poor sleep, high sport load, swelling, or next-day pain can mean the program is too dense even when each exercise looks reasonable on paper. After surgery, or when symptoms are highly irritable, follow the plan set by your surgeon and rehab clinician rather than a generic physiotherapy exercises schedule.
Sample weekly rehab structure
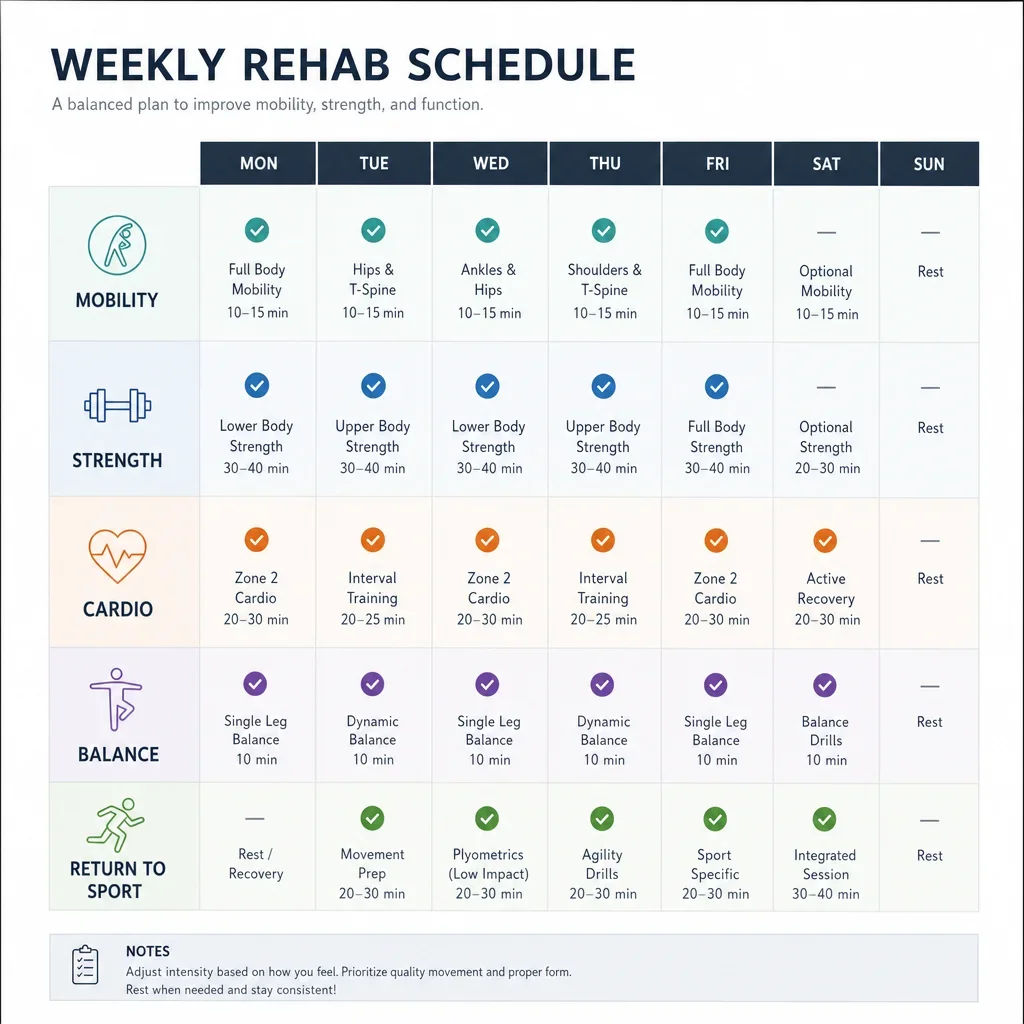
A simple weekly template helps turn a physical therapy exercises list into a routine you can actually follow. An early-stage week may include short daily mobility or activation, 2 to 3 basic strength sessions, and 2 to 5 low-impact cardio sessions depending on tolerance. A later-stage week may include 2 to 4 strength sessions, regular balance or trunk work, and 1 to 2 higher-level functional sessions if impact is appropriate.
Here is a general example for early rehab:
- Daily: 5 to 10 minutes of mobility or activation
- 2 to 3 days: controlled strength work
- 2 to 5 days: bike, pool, walk, or elliptical
- 2 to 4 short blocks: balance or proprioception exercises
Here is a general example for later rehab:
- 2 to 4 days: progressive strength
- 2 to 3 days: low-impact cardio or return-to-run progressions
- 1 to 2 days: return to sport exercises such as landing, deceleration, or agility
- Short daily work: mobility, tissue-specific prep, or movement quality
Think of this like a checklist, not a prescription. If you need a Physical Therapy exercises PDF or a program sheet, the safest version is one built from your assessment findings and updated as you progress.
Return-to-sport progression: from rehab to performance

Pain reduction is not the same as being ready for sport. Return to sport exercises should rebuild strength, confidence, repeated-effort tolerance, movement quality, and sport-specific demand exposure. The path usually moves from controlled strength to plyometrics, then acceleration and deceleration, then cutting, reactive work, and full training exposure when appropriate.
Readiness is usually judged by side-to-side control, movement confidence, tolerance to repeated effort, and whether your sport demands have been reintroduced step by step. A runner may need graded running volume and landing tolerance. A soccer player may need deceleration and cutting. A basketball player may need repeated jumping and directional change. A tennis player may need rotational control and shoulder endurance. A weightlifter may need restored bracing and force transfer before heavy lifts.
If your goal is a safe return to competition, higher-risk cases like ACL recovery or recurrent ankle sprains are where supervised testing adds real value. At our downtown Toronto clinic, that usually means building the program around biomechanics, sport demands, and what your body can actually tolerate now.
Troubleshooting pain, swelling, flare-ups, and form errors

If an exercise flares symptoms, the first fix is usually to reduce range, load, speed, or total volume before stopping all activity. If a movement feels unstable, regress to a supported or bilateral version. If swelling increases after sessions, reduce demand and consider clinician review.
Recurring flare-ups usually mean one of three things: the dosage is too high, the technique is off, or the exercise does not match the diagnosis or phase. Common errors include rushing reps, poor bracing, shifting to the opposite side, shrugging during shoulder work, letting the knee collapse inward, and bouncing through painful range.
A useful rule is that a rehab exercise should look controlled before it looks impressive. Physical therapy exercises with pictures or short videos help because visual feedback often catches form faults that written instructions miss.
Equipment that can make rehab easier or more effective
Simple tools are usually enough. Resistance bands, dumbbells, a step, foam roller, stability ball, balance pad or board, cones, agility ladder, and a slant board all have a place in rehab. The tool matters less than selecting the right exercise, the right dosage, and the right progression.
Bands work well for assisted range, cuff loading, and anti-rotation work. Dumbbells and kettlebells help rebuild strength. A step helps with step-ups, step-downs, and calf work. A balance pad increases proprioceptive challenge. Cones and ladders are useful later for movement patterning and reactive drills. A slant board can help some ankle mobility or calf-loading setups. Fancy equipment is often overused when a simple bodyweight drill would do the job better.
Recovery strategies that support exercise results
Exercise is central, but recovery habits decide how much benefit you get from it. Sleep, stress, pacing, load management, and breathing all affect tissue irritability, coordination, and recovery quality. Doing too little can stall progress. Doing too much can keep symptoms active.
Low-impact cardio during recovery often helps because it maintains fitness without the same joint loading as return to sport work. Common options are stationary bike, pool work, deep-water running, elliptical, and walking progressions when tolerated. The right option depends on the injury site, impact tolerance, and whether the goal is fitness maintenance or return-to-run preparation.
Manual therapy and other adjuncts may help some people feel better or move better for a window, but progressive loading remains the backbone of most sports rehabilitation exercises.
When to book a physiotherapy or sports medicine assessment
Book an assessment when pain persists, progress stalls, the right exercise is unclear, or your goal is to return to running, lifting, court sport, or post-surgical activity safely. That is also the smart next step if generic full body physical therapy exercises are not addressing the actual weak link in your movement.
A good assessment can identify whether your next step is mobility, strength, tendon loading, balance retraining, trunk control, or a true return-to-sport progression. At Focusphysio in downtown Toronto, we use a biomechanics and sports-medicine approach across physiotherapy, chiropractic, and massage therapy to turn a generic exercise list into a plan that fits your injury, your training, and your goals.
FAQ
What are sports therapy exercises?
They are rehab exercises used to restore motion, strength, balance, control, and confidence after injury, surgery, or pain. They can range from early mobility and isometrics to later-stage strength, plyometrics, and sport-specific drills.
What sports therapy exercises can help me recover from an injury or surgery?
The useful category depends on the problem. Early rehab may focus on swelling control, range, breathing, and isometrics. Mid-stage work often adds strength and balance. Late-stage rehab usually adds impact, deceleration, and return-to-sport drills if needed. This page is general information, not a diagnosis or treatment plan.
How often should I do physiotherapy exercises?
Mobility and low-load activation may be done daily, while heavier strength work is commonly done 2 to 4 times per week. Frequency should match soreness, swelling, sleep, and your overall training load.
Can I do sports therapy exercises at home?
Yes, many physical therapy exercises at home are effective for mobility, activation, and basic strength. Home rehab works best when the exercise has been matched to the right diagnosis and stage.
What exercises help with balance and proprioception after injury?
Single-leg stance, supported reach drills, step-down control, perturbation work, and surface or visual changes are common balance and proprioception exercises. They are especially useful after ankle, knee, and hip injuries.
What low-impact cardio can I do while recovering?
Stationary bike, pool work, deep-water running, elliptical, and walking progressions are common options. The safest choice depends on the injured area and how much impact you can tolerate.
What sports therapy exercises are used for ACL rehab?
Common categories include knee extension work, quad activation, gait retraining, single-leg strength, landing mechanics, and later deceleration or cutting drills. Exact exercises and timing depend on surgery details, swelling, strength, and your clinician’s plan.
What exercises help a sprained ankle recover?
Ankle mobility, calf raises, foot control, single-leg balance, and later hopping or agility progressions are common. Repeated giving way or major swelling should be assessed rather than self-managed indefinitely.
When should I stop rehab exercises and see a physiotherapist?
Stop and get assessed if exercise causes sharp pain, repeated instability, increasing swelling, locking, major loss of function, or symptoms that do not settle. Urgent medical care is appropriate for severe weakness, inability to bear weight, bowel or bladder changes, chest pain, or shortness of breath.
Should I use a generic physical therapy exercises PDF?
Use it as a memory aid, not as proof that an exercise is right for you. A generic PDF, online list, or physical therapy exercises with Pictures is only useful if it matches your diagnosis, your capacity, and your phase of healing.
If you are in downtown Toronto and want help turning a general rehab plan into one that fits your body and sport, book an assessment with a licensed clinician who can watch you move and progress the program safely.